e-Surgiroute — Digital Process Mapping for Surgical Pathways
The Context
Surgical site infections remain one of the most common healthcare-associated complications in the NHS. Preventing them requires understanding exactly what happens at every stage of a patient’s surgical journey — from consultant review and decision for surgery through to discharge and follow-up post-discharge — and identifying where practice varies between teams, specialisms, and hospital sites.
At Guy’s and St Thomas’, this work sits with the Surveillance and Innovation Unit within the Directorate of Infection. The unit is responsible for SSI surveillance across multiple surgical specialisms and hospital sites, including Guy’s, St Thomas’, Evelina Children’s Hospital, Royal Brompton and Harefield hospitals.
The unit had developed an effective approach to process mapping over the years: members of the surveillance team would visit departments in person, sit down with clinicians, walk through their procedures, and capture the details in structured spreadsheets. This hands-on method produced thorough, clinically grounded maps — and it worked well within a single specialism or site.
As the team’s ambitions grew — mapping infection prevention pathways across multiple specialisms, multiple hospital sites, and potentially extending the approach to partner trusts — the question became how to scale that same rigour without multiplying the time and physical presence required.
A digital platform was the natural next step: capture the same structured data remotely, from the clinicians themselves, and generate the process maps automatically.
The Brief
The Trust commissioned a web platform to bring this approach into a digital, scalable format. The project was led by the Trust lead for SSI surveillance, with operational support from the wider surveillance team.
The core requirements were defined collaboratively across a series of working sessions:
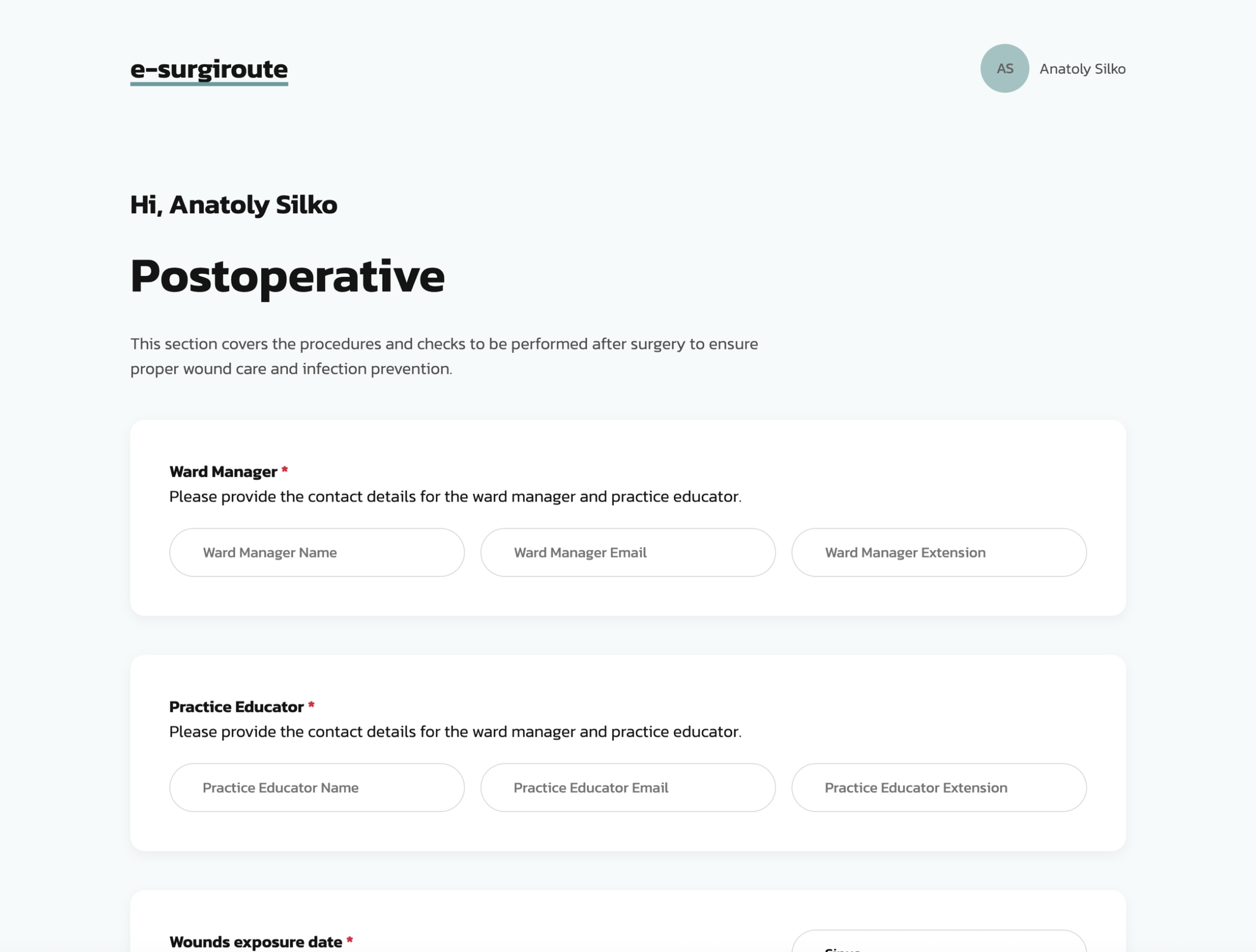
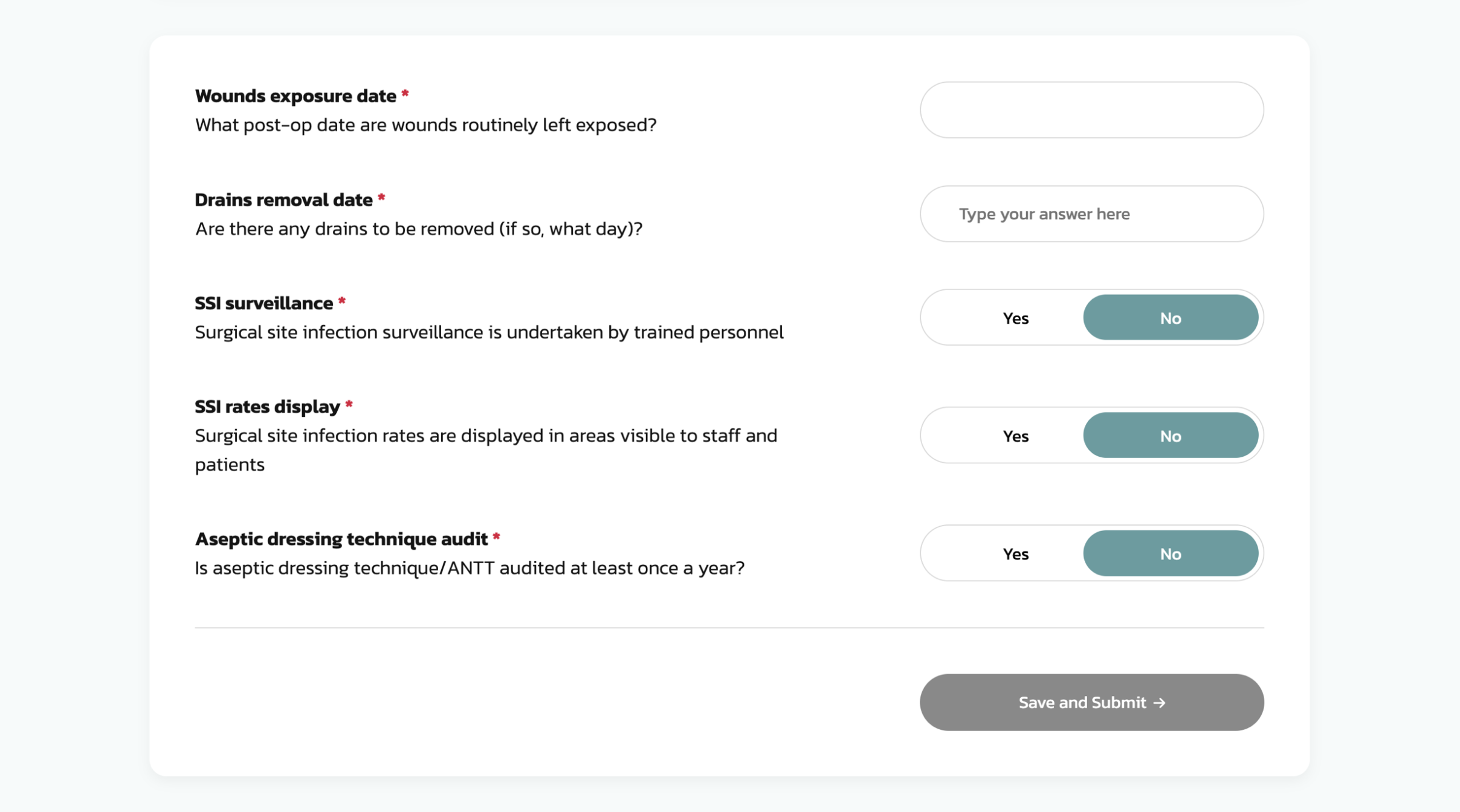
- A dynamic questionnaire system, capable of capturing surgical pathway data across standardised stages — pre-admission, intra-operative, post-operative, and discharge — with each section assignable to different respondents within a specialism. The platform needed to support conditional logic, so that follow-up questions adapted based on previous answers, and multiple input types including yes/no, multi-select, numeric, and free text.
- An invitation-based access model, where clinicians receive a single-use email link to complete their assigned sections without needing to create an account or remember credentials. This was critical for adoption: the platform would be used by busy clinical staff completing a section during a short break, not administrators logging in daily.
- An interactive process map generated automatically from questionnaire responses, visualising the full surgical pathway with aggregated data — which infection prevention measures are in place, which are dominant across respondents, and where practice diverges.
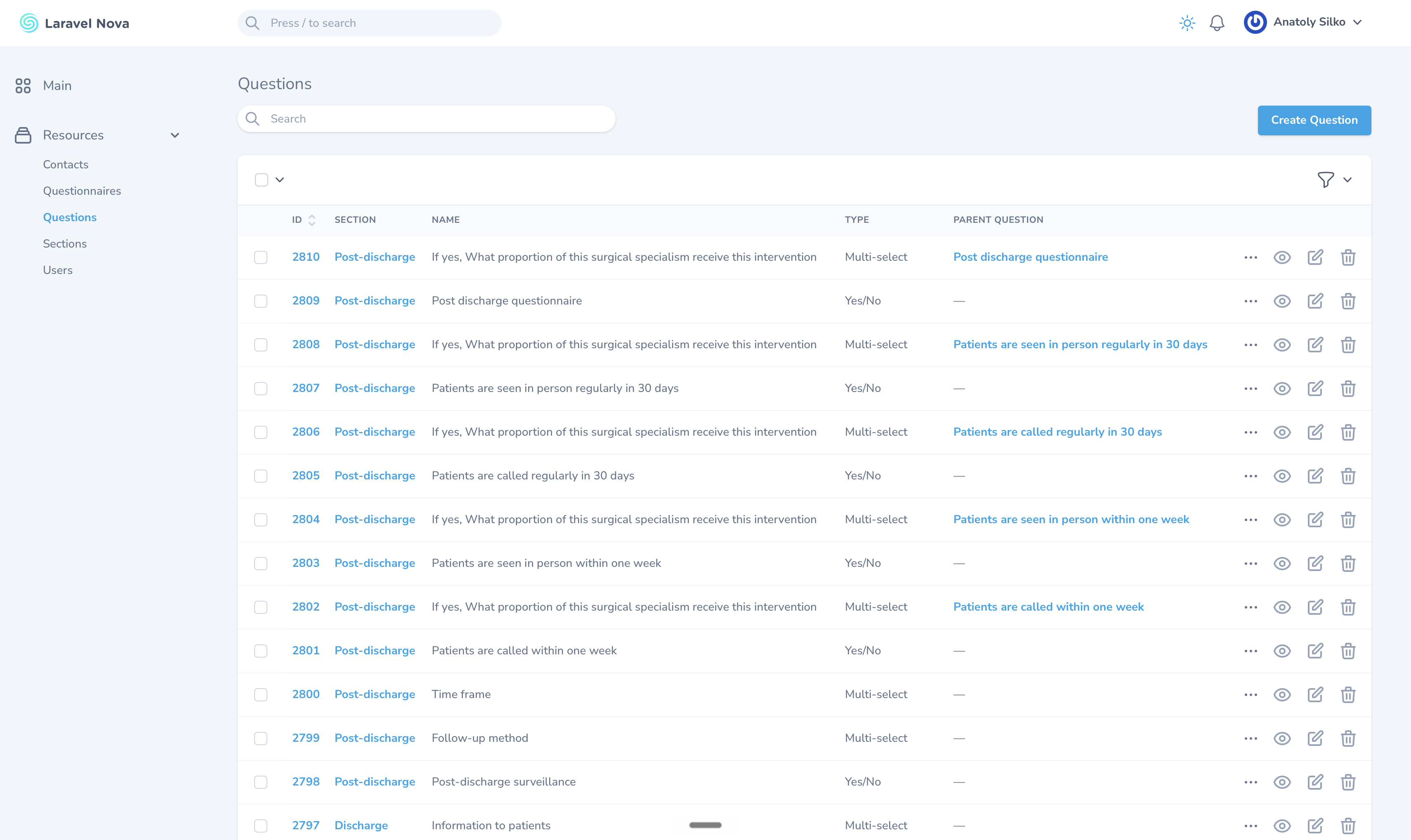
- An admin panel that allowed the surveillance team to manage everything — questions, sections, users, invitations, and results — without developer involvement. The platform needed to be sustainable beyond the initial build: new specialisms, new questions, new hospital sites, all configurable by the team themselves.
The project followed an iterative approach: the proposal outlined an eight-week timeline, but the scope evolved significantly during delivery as the clinical requirements became clearer through hands-on collaboration, particularly around branching logic, process map layout, and the relationship between questionnaire structure and visual output.
Dynamic by Design
The most significant technical decision — and the one that defines the platform’s long-term value — was the data model.
The straightforward approach would have been to hardcode the questionnaire: build fixed forms for each surgical pathway stage, store the responses, and generate a report. That would have been faster to deliver and simpler to build. It would also have been disposable — every new specialism, every revised question, every additional hospital site would require a developer.
Instead, we built a fully dynamic questionnaire engine managed entirely through the admin panel. The data model separates structure from content through six interconnected entities:
A Template is a reusable skeleton — a set of sections and questions that defines a type of surgical pathway mapping exercise. The template for orthopaedics and the template for general surgery share the same underlying structure but can diverge in their questions.
A Questionnaire is a live instance of a template, created when the team is ready to map a specific specialism at a specific site. It inherits the template’s structure but exists independently — responses are collected against the questionnaire, not the template, so multiple mapping exercises can run simultaneously without interference.
Questions belong to templates and carry their own configuration: input type, display text, a short-form alias for process map labels, and position within their section. Sections can be reordered by drag-and-drop in the admin panel. Questions support conditional logic — if a clinician answers “No” to MRSA screening, the follow-up questions about screening protocols are skipped.
Invitations connect users to specific sections of a questionnaire. Each invitation generates a disposable email link — one click to access, no password, no account creation. The surveillance team controls who completes what: a ward manager might be invited to the post-operative section while a theatre nurse handles the intra-operative stage. Invitations track status, expiration, and access level.
Answers are the individual responses, tied to a specific question within a specific questionnaire, attributed to the respondent through their invitation. Auto-saved on input — no submit button until the section is complete, no data lost if the browser closes mid-session.
This architecture means the surveillance team can duplicate a template, rename it for a new specialism, add or remove questions, invite a different set of clinicians, and generate a completely new process map — all without writing a line of code or raising a support ticket. When questions need updating (clinical terminology changes, new national guidelines are issued, a section needs restructuring), the admin makes the change once and it propagates to all active questionnaires instantly.
The Process Map
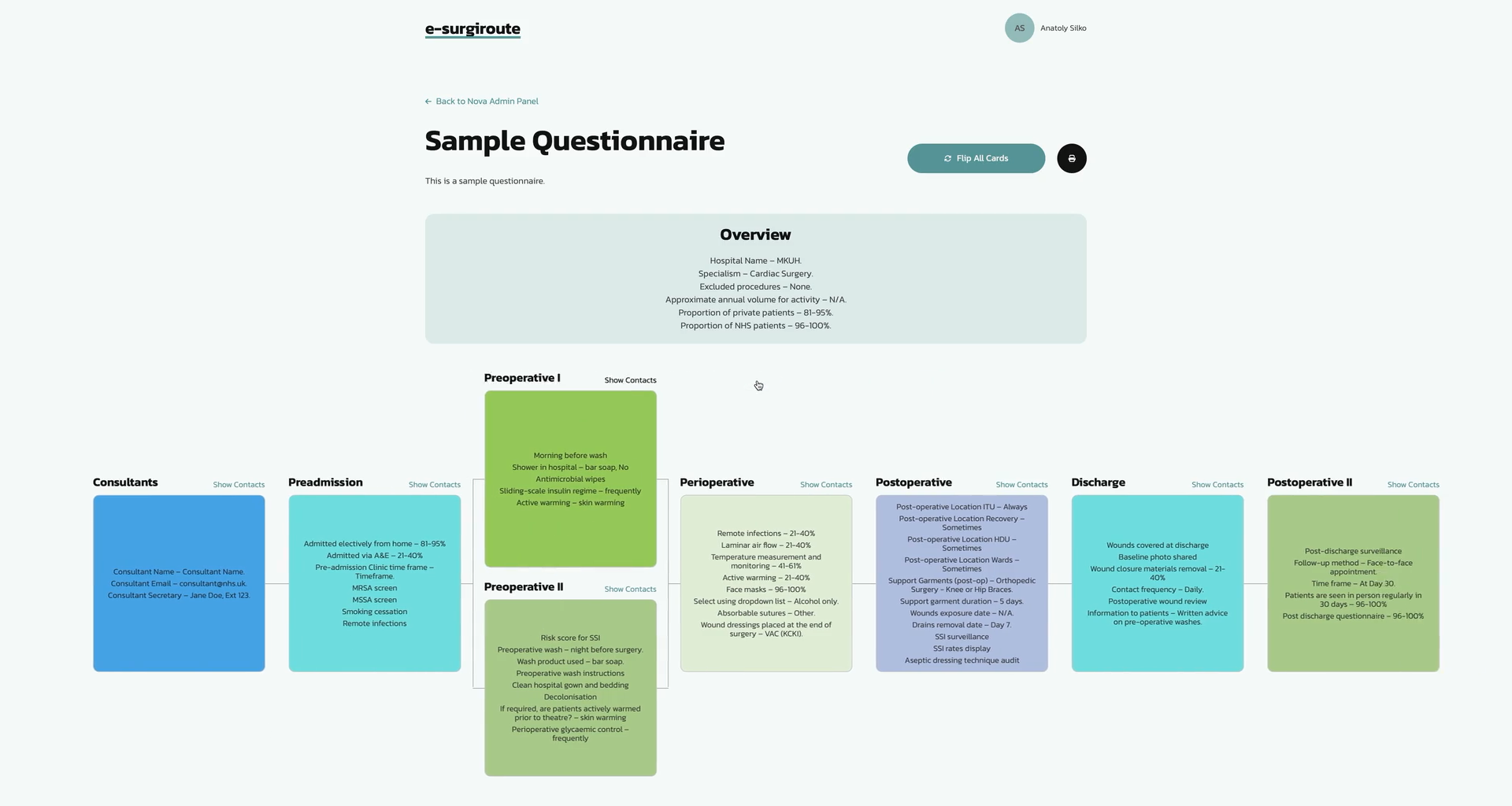
Once respondents complete their sections, the platform aggregates the answers and generates an interactive flowchart — a visual representation of the entire surgical pathway for that specialism, question by question, stage by stage.
Each node on the map corresponds to a question. Where the question has a dominant answer across respondents, the map highlights it. Where practice is split — say, 50/50 on whether a particular antibiotic prophylaxis protocol is followed — the visualisation reflects that ambiguity, giving the surveillance team an immediate signal of where standardisation may be needed.
The map is structured around the surgical pathway stages: pre-admission (patient sources, MRSA screening, HbA1c collection), intra-operative (skin preparation, antibiotic prophylaxis, suture type, dressings, gloving practice), post-operative (ICU, HDU, ward pathways, monitoring protocols), discharge, and post-discharge. Sections are collapsible, so the team can focus on a single stage or view the full pathway end-to-end.
A compressed view was developed alongside the detailed flowchart — a mode that strips out the proportional breakdowns and displays only the confirmed practices at each stage. This was a direct response to clinical feedback: the detailed view is powerful for audit-style analysis, but for day-to-day process mapping, clinicians need a clean overview of what happens at each stage, not a statistical breakdown.
Both views are printable. The print function strips headers, footers, and navigation elements, outputting only the pathway content. Cards within the map are flippable — one side shows the procedure or practice, the reverse shows the responsible contact or department — and a “flip all” button allows the entire map to be printed with contacts visible, creating a reference document that can be taken into a ward or theatre.
Stack and Infrastructure
The platform was built on Laravel with a Vue.js frontend, MySQL database, and deployed on a DigitalOcean droplet — the same proven stack used across multiple Rocking Tech projects, including Reflecta for Buckinghamshire New University.
The admin panel uses Laravel Nova, providing a customisable interface for managing every entity in the system — templates, sections, questions, questionnaires, invitations, users, and answers. Nova’s built-in filtering, search, and batch actions reduce the overhead of managing what quickly becomes a large dataset as multiple specialisms are mapped simultaneously. Data can be exported to Excel directly from the admin panel for offline analysis.
Authentication for respondents uses disposable email links — a magic-link approach that eliminates the friction of account creation for clinical staff who may interact with the platform once or twice per mapping exercise. Admin users authenticate through a standard login with session management.
The frontend is fully responsive and touch-optimised, built to work on the devices available in NHS settings — including Microsoft Edge, the Internet Explorer successor mandated as the default browser across the Trust. Input types are designed for speed: large tap targets for multi-select options, +/− buttons for numeric inputs, and real-time validation to catch errors before submission.
Security follows standard web application practices: SSL encryption, SSH access, session management, and CAPTCHA on public-facing forms. The platform handles no patient-identifiable data — it captures infection prevention practices, not patient records — which simplified the data governance requirements significantly.
Hosting runs on a single DigitalOcean droplet with automated backups, managed by Rocking Tech. The infrastructure cost is minimal, which matters for a project funded through NHS operational budgets rather than commercial revenue.
The Outcome
The platform was delivered and deployed at e-surgiroute.uk, giving the Surveillance and Innovation Unit a digital, repeatable alternative to the manual process mapping approach.
The full surgical pathway questionnaire — covering over 500 structured questions across nine sections from pre-admission through to post-discharge — is now configured and managed by the surveillance team through the admin panel, without needing code changes.
The team independently creates questionnaires for different specialisms and hospital sites, configures section-level questions, issues invitations to clinical respondents, and reviews the resulting process maps. Multiple questionnaires have been configured across the platform, including setups for specific surgical specialisms and hospital sites within the Trust.
Clinical staff across the unit were given access to the platform over a nine-month period, including clinical nurse specialists from the Central Digital Wound Hub and colleagues from the wider Directorate of Infection. Their feedback shaped iterative improvements throughout the process: a real-time progress bar for long questionnaires, personalised invitation messages, refined print layouts for the process map, and content adjustments to align terminology with clinical practice — brand names for surgical preparations, clearer distinctions between skin prep and hand hygiene protocols, and updated suture and dressing classification options.
The architecture was built to scale beyond a single unit. The dynamic data model means any new specialism, any new hospital site, and any future partner trust can be onboarded by duplicating a template and configuring the questions — no code changes, no developer dependency. That was a deliberate design decision from the outset, and it is what gives the platform value beyond its initial deployment.
What’s Next
The platform was designed from the outset to extend beyond a single unit and a single trust. The dynamic architecture — templates, configurable questions, invitation-based access — means any NHS organisation running surgical pathway mapping or SSI surveillance can be onboarded without structural changes to the platform.
Future iterations could introduce comparative reporting across specialisms and hospital sites, benchmarking tools for infection prevention compliance, and integration with existing NHS data systems. The foundation is in place; what comes next depends on where the clinical need takes it.